
肾健康与营养(专业版)
如果要保持健康长期的生活目标,维护肾脏健康是至关重要的。肾脏是身体的关键过滤器之一,起着排除废物、支持体液电解质平衡,以及调节血压和维持造血功能等。
英文名称:Kidney health
概述
如果要保持健康长期的生活目标,维护肾脏健康是至关重要的。肾脏是身体的关键过滤器之一,起着排除废物、支持体液电解质平衡,以及调节血压和维持造血功能等。近年来,慢性肾病发病率在中老年人中快速增长,与糖尿病和高血压等疾病迅速增加有关。此外,肾脏健康的最大威胁之一还来自于人们日常使用的止痛发烧药和抗炎药,过量或长期使用都可对肾脏产生损伤。调整饮食和生活方式,以及补充必要的营养和草本制剂,可支持肾脏功能,并预防或延缓慢性肾病,提高生命品质。肾脏功能简介
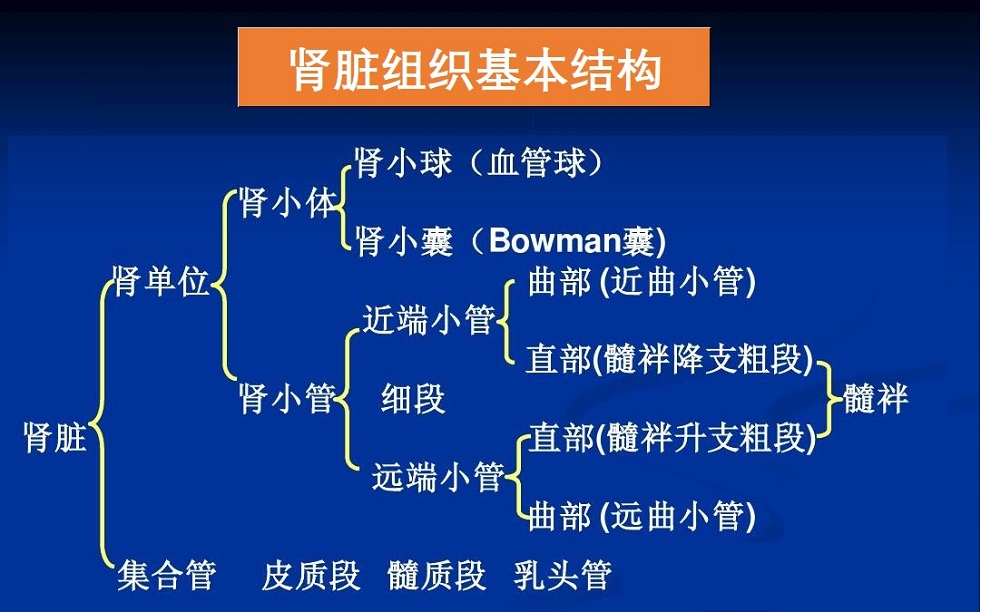
肾脏是人体主要排泄器官,其将血液中的代谢废物过滤分解形成尿液输出体外。此外,肾脏还调节体液、维持水电解质酸碱平衡等,发挥内分泌器官作用,参与血压、造血和钙鳞代谢等调节。- 生成尿液、排泄代谢物:人体新陈代谢产生的多种废物,绝大部分通过肾小球血滤过、肾小管分泌,随尿液排出体外。肾小球每分钟滤过1200ml血液;人体正常排尿1-2000ml/天。
- 维持体液和水电解质酸碱平衡:通过肾小球的滤过,肾小管的重吸收及分泌功能,排出体内多余的水分,调节酸碱平衡,维持机体细胞内环境稳定。
- 维持血液PH值相对恒定,包括肺部(调节二氧化碳)和肾小管(分泌酸和吸收碳酸氢盐)
- 内分泌和调节功能:
- 调节血压:肾脏分泌肾素升高血压,而分泌前列腺素则降低血压。
- 促红细胞生成素:刺激骨髓造血、生成红血细胞。
- 活化维生素D3,调节钙磷代谢。维生素D在体内必须经肾脏转变为1,25-2羟维生素D3,才能发挥其生理作用,维生素D受体遍布全身,包括大脑等。
- 降解多种内分泌激素,如胰岛素、胃肠激素等。如果肾功能不全,则可引起代谢紊乱。
- 毒素、药物代谢:肾小管的细胞含有许多与肝细胞相同的解毒酶,支持机体解毒功能。
- 葡萄糖生成(糖异生):只有肝、肾和小肠能够从人体中的非糖化合物产生葡萄糖。过夜禁食后,肾脏产生约四分之一的葡萄糖释放到血液中。胰岛素抑制肾脏葡萄糖生成,而肾上腺素刺激糖异生。
影响肾脏健康主要因素
- 高血糖:糖尿病是慢性肾病产生的主要原因,大约30%糖尿病患者可并发糖尿病肾病。糖化血红蛋白和晚期糖基化终产物(AGEs)是糖尿病肾病形成和发展的主因。前者主要损害微血管,后者具有促炎和促氧化作用,损伤肾小球而导致慢性肾病。
- 高血压:是慢性肾脏疾病的第二主要原因。高血压可损害肾脏中的血管而影响肾过滤。受损的肾脏因此不能调节血压,而进一步恶化高血压。
- 肥胖症:研究表明,肥胖是慢性肾病发病及严重程度的独立危险因素。
- 代谢综合征和胰岛素抵抗:与高血压、空腹血糖高和高甘油三酯等相关,并同时伴发胰岛素抵抗,这是肾脏疾病进展的独立预测因素。可引起肾脏微血管氧化应激、炎症反应,降低肾小球滤过率、尿蛋白增加等。
- 甲状腺功能减退:导致肾功能紊乱,如肾血流减少、过滤和钠重吸收,与慢性肾病进展有关。
- 年龄增长影响:一般估计,老年群体肾功能障碍或慢性肾病发病率15-35%之间。
- 某些药物损伤肾脏,最常见的是由于长期或过度使用,如非甾体抗炎止痛药(NSAIDs)。
- NSAIDs可抑制肾脏前列腺素分泌、血液在肾脏流动,影响肾小球滤过,在老年和慢性肾脏疾病中尤其明显。
- 抗生素:包括万古霉素、氨基糖苷类、青霉素、头孢菌素、利福平和氟喹诺酮类等,甚至可能引起急性肾损伤。
- 化疗药:肾毒性是顺铂、阿霉素和奥沙利铂等化疗药的常见副作用。许多化疗药物通过肾代谢和排泄,使肾脏暴露于其毒性作用中。
- 酸性饮食:肾脏主要作用之一是排泄过量的酸,可保持血液的pH在窄的、微弱的碱性范围内,以支持正常的代谢功能。当肾脏衰老并丧失一些功能时,在消除这种酸度方面效率降低,结果血液酸度增加。这反过来,也进一步损害肾脏。饮食减少红肉类,及富含蔬菜、水果等可减少酸性物质,或补充碳酸氢钠也有助于防止低度全身代谢性酸中毒。
- 肾上腺功能障碍:肾上腺功能可对肾功能产生深远的影响。皮质醇过高可导致水和钠滞留,引起高血压和肾结石产生。
- 尿崩症:由于抗利尿激素的产生或响应失败,肾脏不能有效地再吸收水。尿崩症可以是先天性或获得性的。
- 肠道微生物与肾健康:当肠道菌群失衡导致肠道通透性增加(如肠漏)后,细菌和毒素进入血液中,促进慢性肾病形成和发展。
肾脏主要疾病及影响
- 慢性肾病(CKD):它是肾功能进展性下降的疾病,肾小球滤过逐渐降低,引起血液中废物和毒素增加,以及代谢性酸中毒和贫血等。糖尿病、高血压是CKD主要原因。更多相关内容可参阅本网有关专文慢性肾病 >>。
- 急性肾损伤:通常是指几小时到几天内发生的肾功能的快速衰竭。它可由肾脏本身健康原因、进入肾脏的血液流量减少(肾前性原因),以及下尿路损伤或感染导致尿毒症毒素进入肾脏(肾后原因)引起。
- 肾前原因主要如:严重失血、脱水、心力衰竭、肺栓塞、败血症、过量的血钙和一些药物如非甾体抗炎药(NSAIDs)等。
- 肾后原因主要如:尿道可能被输尿管、膀胱或尿道由石头、肿瘤、前列腺增生,创伤或感染阻塞而损伤。
- 多种疾病如:自体免疫疾病、感染、淋巴瘤,某些药物和导致快速组织破坏的疾病等也可以直接损伤到肾脏。
- 肾结石:是常见的肾脏疾病之一,常见类型包括:
- 草酸钙结石:为最常见的肾结石类型约占76%,主因是高尿钙水平。
- 磷酸钙:由高尿酸,酸性尿和痛风或代谢综合征引起。
- 鸟粪石:主要由泌尿道感染引起,女性居多;以及与胱氨酸转运的遗传疾病相关。
肾健康的综合干预
选项可包括如下:饮食与生活方式
- 关注非甾体抗炎药NSAIDs:应使用最低剂量,且避免长期服用。
- 研究表明,使用对乙酰氨基酚(止痛药主要成分)和其他NSAIDs与肾脏疾病的风险相关。
- 阿司匹林,作为最常用的NSAIDs药物之一,其对肾脏健康影响证据存在异议,应遵循医嘱。
- 经常服用NSAIDs群体,尤其是60岁以上老年人,宜定期检查肾功能状况。
- 限制动物蛋白、精制碳水化合物(米面类)饮食,增加蔬菜、水果和全谷类食物。
- 限制盐分、甜饮料和高脂肪饮食,适量增加鱼类、坚果等摄入。甜饮料和许多甜品主要使用果糖浆,可增加尿酸性,对肾脏健康不利。
- 保持合适的身体锻炼,有氧运动。
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于维持肾健康营养和草本补充剂,主要包括如下:
1.辅酶Q10:
一项针对55名透析前患者的小型研究,评估了受试者血液中氧化应激标志物和辅酶Q10(CoQ10)的水平。在肌酐清除率轻度下降的受试者中,氧化应激标志物丙二醛水平升高,辅酶Q10水平降低。这两个结果显著相关,作者得出结论,氧化应激是肾脏疾病进展的早期事件1。
辅酶Q10有益于肾脏健康的另一个重要路径是帮助保持血压水平健康。一项严肃的文献分析汇集并分析了三项独立试验的数据,发现补充辅酶Q10 4-12周可使收缩压和舒张压分别降低11mmHG和7mmHG,具有高度临床和统计学意义。分析研究中使用的CoQ10剂量范围为每天100-120mg2。在一项针对2型糖尿病患者的随机对照试验中,连续12周每天200mg辅酶Q10可显著降低收缩压和舒张压,分别降低6.1mmHg和2.9mmHg。衡量长期血糖控制的血红蛋白A1c水平也下降了0.37%3。这些发现表明CoQ10在保护肾脏健康方面发挥着重要作用,因为高血压和血糖升高都是肾脏疾病的重要危险因素。
此外,动物研究表明,辅酶Q10可以保护肾组织免受多种肾毒性药物的影响,包括庆大霉素、顺铂和环孢菌素4-7。
2.维生素D:
已知肾脏在将维生素D转化为活性形式方面发挥作用,肾脏疾病会导致维生素D缺乏。维生素D也可能对肾脏产生保护作用:动物模型研究表明,活性形式的维生素D可以抑制肾脏炎症、纤维化和细胞死亡;并防止顺铂的毒性。在人类中,这种治疗可以减少尿液中的蛋白质损失并改善免疫功能8。在观察性研究中,接受骨化三醇或合成维生素D类似物(不需要肾脏激活的维生素D活性形式)治疗的CKD和透析患者的心血管和全因死亡率降低9。在接受合成维生素D类似物或骨化三醇治疗的CKD患者中进行的临床试验显示,尿液中蛋白质损失较低,白蛋白与肌酐的比率较低,心脏功能改善10-12。
3.L肉碱:
接受肾透析的患者可能会出现功能性肉碱缺乏,即透析相关性肉碱紊乱,这种情况包括对红细胞生成素治疗反应不佳的贫血;透析期间低血压;心肌病;以及肌肉功能障碍,其主要症状是全身疲劳。这种疾病是由于在透析期间去除大量的肉碱引起的。美国国家肾脏基金会(NKF)建议在每次透析后静脉注射20mg/公斤体重的L肉碱来治疗与透析相关的肉毒碱紊乱症状13。
L肉碱可能对透析患者有额外的益处:一项涉及1734名肾透析患者的49项临床试验的荟萃分析发现,服用L肉碱的患者C反应蛋白和LDL显著降低。在该文献综述中,37项试验采用静脉注射L肉碱,12项试验采用口服L肉碱14。
4.欧米伽3脂肪酸:
在几项针对高血压患者的临床试验中,鱼油中的Omega-3脂肪酸已被证明可显著降低血压(CKD的风险因素)15,16。在一项双盲试验中,以每天4g的剂量补充Omega-3脂肪酸可降低CKD患者的血压17。其他证据表明,ω-3脂肪酸可以减少CKD患者的蛋白尿,并减少透析患者的炎症和甘油三酯。在低饱和脂肪的植物性饮食中多吃油性鱼类可能有益于CKD患者或有患CKD风险的患者18。一项针对3000多人的研究表明,在那些更坚持地中海式饮食的人中,更多的长期鱼类消费与肾功能的改善有关19。
5.益生菌和益生元:
改善消化道中细菌和微生物的平衡在预防尿毒症毒素的形成和帮助清除血液中的尿毒症毒素方面显示出了前景。由于这些毒素对肾功能产生负面影响,它们与CKD的肾损伤有关20-23。啮齿动物研究表明,益生元(有利于益生菌的膳食纤维)能够预防CKD相关的胰岛素抵抗。这种能力是由尿毒症毒素积累减少引起的24,25。目前正在中重度CKD患者中进行益生菌和益生元组合的试验26。
6.N乙酰半胱氨酸:
N-乙酰半胱氨酸(NAC)是一种含硫化合物,有助于抵消重金属毒性的破坏作用27,28。在动物模型中,NAC增强了肾脏对铬和铅的排泄,并降低了肾脏中汞的浓度29。在对盐敏感性高血压大鼠模型中,NAC可能通过增强肾脏谷胱甘肽来减少肾脏蛋白质损失和肾小管损伤,并改善肾小球滤过率和肾血流量30。
在一组24名血液透析患者中,连续三个月每天两次600mg NAC可显著降低一些血清炎症标志物,包括白细胞介素-6和C反应蛋白。研究人员表示,“这表明[终末期肾病]患者可能受益于NAC的抗炎作用”31。其他证据表明,NAC可能有助于治疗儿童化疗药物异环磷酰胺(Ifex)引起的肾毒性32。
7.镁:
高血压会严重损害肾脏健康33,镁已被证明在每天摄入500-1000mg的水平下可以降低血压34。此外,镁可以改善降压药物的性能,并可能改善血管壁内皮细胞的功能34-36。镁缺乏与糖尿病和代谢综合征有关,这两种疾病都是肾脏疾病的危险因素37-40。此外,柠檬酸镁钾已被研究作为一种尿碱化剂,以防止肾结石的形成41。
然而,肾脏是过量镁从体内排出的主要途径。当eGFR降至约30mL/min以下时,镁水平可能增加。目前还不确定较轻的肾损伤(如eGFR>30)会产生什么影响,因此患有肾脏疾病的患者在服用镁之前应咨询其医疗保健提供者42,43。
8.维生素E:
在接受冠状动脉成像研究的个体中,用350mg α-生育酚或300 mg γ-生育酚以及静脉盐水进行7天的预防性治疗,降低了造影剂诱导的急性肾损伤的发生率44。与对照组相比,补充维生素E、普伐他汀和降低同型半胱氨酸的B族维生素叶酸、B6和B12的组合,改善了心血管健康指标,减少了肾脏白蛋白损失45。在一项针对非糖尿病CKD患者的试点试验中,维生素E减少了不对称二甲基精氨酸,这是一种内皮型一氧化氮合酶抑制剂,在CKD患者中升高,是一种拟议的心血管风险因素46。
9.钾(柠檬酸钾):
柠檬酸钾和碳酸氢钠一样,是一种碱盐47,48。在多囊肾病的动物模型中,它成功地保存了GFR,显然是通过其碱化作用49。
在一项针对老年人的研究中,每天摄入9g碳酸氢钾可以减轻蛋白质摄入对尿液的影响50。
10.活性维生素B6(5'-磷酸吡哆醇):
5’-磷酸吡哆醇(P5P)是维生素B6的一种形式51。它是吡哆胺的代谢产物,吡哆胺是维生素B6的一种形式,是晚期糖基化终产物(AGE)形成的有效抑制剂,这是糖尿病肾病的特征之一。
正在研究吡哆胺对糖尿病肾病患者维持肾功能的作用52。P5P本身可能有助于维持糖尿病患者的肾脏健康;在糖尿病动物模型中,施用P5P抑制AGE的形成、尿液蛋白损失、肾组织的纤维化和糖尿病肾病的发展53。
以下是基于临床前研究对肾脏有益的营养物:
1. 水飞蓟素:
水飞蓟素具有抗氧化、阻断毒素的特性,被认为是一种安全且耐受性良好的天然化合物54,55。
在实验模型中,水飞蓟素当以相当于成人每天约220mg至2.2g的剂量给药时,可以保护肾细胞和大鼠肾脏免受毒素过量引起的损伤56,57。类似地,当以相当于成人约567mg的剂量给予大鼠时,水飞蓟素可保护大鼠免受缺血再灌注损伤,这是一种促氧化状态,也是急性肾损伤的主要原因58。此外,研究人员发现水飞蓟素可以完全防止在葡萄糖浓度升高的情况下培养的肾细胞损伤,同时阻断氧化应激标志物的产生59。
水飞蓟素对几种肾毒性药物也有保护作用,特别是顺铂和阿霉素。这是两种最有效的化疗药物,但由于其产生的氧化损伤和严重炎症,也是对肾脏损伤最大的两种药物60,61。几个研究小组发现,在动物模型中,水飞蓟素及其成分可以减少甚至完全预防这些药物引起的肾脏损伤62-64。
2.绿茶:饮料或提取物形式的绿茶,以及分离的绿茶多酚(EGCG),在动物模型中降低了庆大霉素、顺铂和环孢菌素药物的肾毒性。这些研究中使用的剂量范围为成人约1.1g至约3.4g绿茶的当量65-67。此外,绿茶被证明可以预防糖尿病肾病大鼠的肾脏损伤68。EGCG与α-硫辛酸联合降低了AGEs在人类肾细胞中诱导的炎症变化69。
3.姜黄素:姜黄素已被证明可以降低庆大霉素、顺铂、阿霉素、氯喹(Aralen)和环孢菌素药物的肾毒性70-73,以及动物模型中的重金属镉和汞74。在糖尿病肾病的动物模型中,相当于成人约1100mg的姜黄素剂量可防止肾脏疾病的进展75。
4.白藜芦醇:白藜芦醇是一种天然的多酚类植物化学素。白藜芦醇可能有望通过调节与肾脏损伤有关的几种细胞途径来治疗CKD。例如,白藜芦醇抑制核因子κB(NF-κB),这是参与肾脏损伤的炎症过程的主要协调物。此外,白藜芦醇是氧化应激的有效抑制剂,也是导致肾脏损伤的重要因素76。在动物模型中,白藜芦醇治疗已被证明可以抑制肾脏氧化应激,改善肾循环,并提高败血症相关急性肾损伤的存活率77。白藜芦醇还被证明可以减少大鼠肾脏的缺血再灌注损伤78。
在糖尿病大鼠中,白藜芦醇剂量相当于成人正常化肌酸酐清除率(肾功能的一种衡量标准)的约56mg,减轻了肾组织中氧化损伤的几种标志物,并提高了抗氧化酶和维生素C和E的水平79。在实验室和动物模型中,约90-227mg的白藜芦醇人体等效剂量已被证明可以减少因顺铂、阿霉素、庆大霉素或砷毒性引起的急性肾损伤80-82。动物模型的其他证据表明,白藜芦醇可以预防药物诱导的和败血症相关的肾损伤,以及与输尿管梗阻相关的肾损害83。
5.α-硫辛酸:
含硫化合物可与有毒重金属形成络合物。α-硫辛酸是一种含硫抗氧化剂,在实验室模型中已被证明有助于清除许多有毒金属,如镉、铅、钴和镍84。α-硫辛酸注射液减少了镉催化的氧化应激,并增加了大鼠肾脏中抗氧化酶过氧化氢酶的活性85。α-硫辛酸在动物模型中降低化疗药物如顺铂和阿霉素的肾毒性86,87,并有助于在糖尿病肾病动物模型中保护肾功能88。它还可以在动物模型中预防败血症引起的急性肾损伤89。
6.牛磺酸:牛磺酸是一种含硫氨基酸。在动物模型中,牛磺酸已被证明可以降低镉、对乙酰氨基酚和与糖尿病相关的AGEs引起的肾毒性90。动物模型的证据表明,牛磺酸可以保护肾组织免受酒精代谢诱导的损伤91。另一项动物实验表明,牛磺酸可以保护大鼠肾脏免受21天尼古丁注射造成的损伤。本研究中使用的牛磺酸剂量相当于成年人约567mg92。
7.精氨酸:精氨酸是一氧化氮(NO)的天然前体,NO是一种促进血液流动的化合物,在CKD患者中经常缺乏。这种缺乏可能是慢性受损肾脏中精氨酸合成无效的结果。在高血压大鼠模型中补充精氨酸可以改善内皮功能93。
8.苯磷硫胺:苯磷硫胺是硫胺素(维生素B1)的一种脂溶性形式,可抑制AGEs的形成。苯磷硫胺因其减轻高血糖对神经系统、肾脏和眼睛影响的能力而受到研究,主要在实验室和动物身上进行94。在动物中,已经证明在每天约795mg至约1100mg的人类当量的剂量范围内减少肾脏中AGE的形成和含量95.96;腹膜透析期间防止肾脏损伤96;并减少化疗药物顺铂的肾毒性作用97。在患有糖尿病的啮齿类动物中,苯磷硫胺抑制微量白蛋白尿的发展98。
更多内容可点击其个性化的综合干预方案如下:
以及参阅本网如下专文的有关内容:
参考文献:
1. Gazdíková K et al. Oxidative stress and plasma concentrations of coenzyme Q10, alpha-tocopherol, and beta-carotene in patients with a mild to moderate decrease of kidney function. Nephron. 2001;88(3):285
2. Ho MJ et al. Blood pressure lowering efficacy of coenzyme Q10 for primary hypertension. Cochrane Database Syst Rev. 2009;(4):CD007435
3. Hodgson JM et al. Coenzyme Q10 improves blood pressure and glycaemic control: a controlled trial in subjects with type 2 diabetes. Eur J Clin Nutr. 2002;56(11):1137–42
4. Upaganlawar A et al. Modification of biochemical parameters of gentamicin nephrotoxicity by coenzyme Q10 and green tea in rats. Indian J. Exp. Biol. 2006;44(5):416–8.
5. Fouad AA et al. Coenzyme Q10 treatment ameliorates acute cisplatin nephrotoxicity in mice. Toxicology. 2010;274(1-3):49–56
6. Sato T et al. Effect of reduced form of coenzyme Q10 on cyclosporine nephrotoxicity. Exp Clin Transplant. 2013;11(1):17–20
7. Ishikawa A et al. Beneficial effect of ubiquinol, the reduced form of coenzyme Q10, on cyclosporine nephrotoxicity. International braz j urol. Mar-Apr 2012;38(2):230-234; discussion 234.
8. Kim CS et al. Vitamin D and chronic kidney disease. Korean J Intern Med. 2014;29(4):416
9. Zheng Z et al. Vitamin D supplementation and mortality risk in chronic kidney disease: a meta-analysis of 20 observational studies. BMC nephrology. 2013;14:199.
10. Zoccali C et al. Paricalcitol and endothelial function in chronic kidney disease trial. Hypertension. Nov 2014;64(5):1005-1011.
11. Moe SM et al. A randomized trial of cholecalciferol versus doxercalciferol for lowering parathyroid hormone in chronic kidney disease. Clinical journal of the American Society of Nephrology. Feb 2010;5(2):299-306.
12. Wesseling-Perry K et al. Is replacement therapy with nutritional and active forms of vitamin D required in chronic kidney disease mineral and bone disorder? Current opinion in nephrology and hypertension. Jul 2009;18(4):308-314.
13. Eknoyan G. Obesity and chronic kidney disease. Nefrologia: publicacion oficial de la Sociedad Espanola Nefrologia. 2011;31(4):397-403.
14. Chen Y et al. L-Carnitine supplementation for adults with end-stage kidney disease requiring maintenance hemodialysis: a systematic review and meta-analysis. American Journal of Clinical Nutrition. 2014;99(2):408–22
15. Hartweg J et al. Meta-analysis of the effects of n-3 polyunsaturated fatty acids on haematological and thrombogenic factors in type 2 diabetes. Diabetologia. 2007;50(2):250–8
16. Geleijnse JM et al. Blood pressure response to fish oil supplementation: metaregression analysis of randomized trials. J. Hypertens. 2002;20(8):1493–9
17. Mori TA et al. The effects of [omega]3 fatty acids and coenzyme Q10 on blood pressure and heart rate in chronic kidney disease: a randomized controlled trial. J. Hypertens. 2009;27(9):1863–72
18. Huang X et al. Dietary fat modification in patients with chronic kidney disease: n-3 fatty acids and beyond. Journal of nephrology. Nov-Dec 2013;26(6):960-974.
19. Chrysohoou C et al. Adherence to the Mediterranean diet is associated with renal function among healthy adults: the ATTICA study. Journal of renal nutrition. May 2010;20(3):176-184.
20. Montemurno E et al. What Would You Like to Eat, Mr CKD Microbiota? A Mediterranean Diet, please! Kidney & blood pressure research. Jul 29 2014;39(2-3):114-123.
21. Ramezani A, et al. The gut microbiome, kidney disease, and targeted interventions. Journal of the American Society of Nephrology. Apr 2014;25(4):657-670.
22. Evenepoel P et al. Uremic toxins originating from colonic microbial metabolism. Kidney international. Supplement. Dec 2009(114):S12-19.
23. Vitetta L et al. From the gastrointestinal tract (GIT) to the kidneys: live bacterial cultures (probiotics) mediating reductions of uremic toxin levels via free radical signaling. Toxins. Nov 2013;5(11):2042-2057.
24. Soulage CO et al. Protein-bound uremic toxins...new targets to prevent insulin resistance and dysmetabolism in patients with chronic kidney disease. Journal of renal nutrition. Nov 2013;23(6):464-466.
25. Koppe L et al. p-Cresyl sulfate promotes insulin resistance associated with CKD. Journal of the American Society of Nephrology. Jan 2013;24(1):88-99.
26. Rossi M et al. SYNbiotics Easing Renal failure by improving Gut microbiologY (SYNERGY): a protocol of placebo-controlled randomised cross-over trial. BMC nephrology. 2014;15:106.
27. Patrick L. Lead toxicity part II: the role of free radical damage and the use of antioxidants in the pathology and treatment of lead toxicity. Altern Med Rev. 2006;11(2):114–27
28. De la Fuente M et al. Sulfur-containing antioxidants increase in vitro several functions of lymphocytes from mice. International immunopharmacology. Jun 2011;11(6):661-669.
29. Samuni Y et al. The chemistry and biological activities of N-acetylcysteine. Biochim Biophys Acta. 2013;1830(8):4117–29
30. Tian N et al. N-Acetylcysteine improves renal dysfunction, ameliorates kidney damage and decreases blood pressure in salt-sensitive hypertension. J. Hypertens. 2006;24(11):2263–70
31. Saddadi F et al. The effect of treatment with N-acetylcysteine on the serum levels of C-reactive protein and interleukin-6 in patients on hemodialysis. Saudi journal of kidney diseases and transplantation. Jan 2014;25(1):66-72.
32. Hanly L et al. N-acetylcysteine rescue protocol for nephrotoxicity in children caused by ifosfamide. Journal of population therapeutics and clinical pharmacology. 2013;20(2):e132-145.
33. Rasu RS et al. Treatment of hypertension and diabetes mellitus in patients with chronic kidney disease: a review. Expert opinion on pharmacotherapy. Oct 2007;8(15):2543-2551.
34. Houston M. The role of magnesium in hypertension and cardiovascular disease. Journal of clinical hypertension (Greenwich, Conn.). Nov 2011;13(11):843-847.
35. Barbagallo M et al. Oral magnesium supplementation improves vascular function in elderly diabetic patients. Magnesium research : official organ of the International Society for the Development of Research on Magnesium. Sep 2010;23(3):131-137.
36. Kisters K. Oral magnesium supplementation improves borderline hypertension. Magnesium research : official organ of the International Society for the Development of Research on Magnesium. Mar 2011;24(1):17; author reply 18.
37. Kurella M et al. Metabolic syndrome and the risk for chronic kidney disease among nondiabetic adults. Journal of the American Society of Nephrology. Jul 2005;16(7):2134-2140.
38. Kabir MS et al. Prevalence of risk factors of chronic kidney disease in adults. Mymensingh medical journal : MMJ. Oct 2012;21(4):605-610.
39. Chaudhary DP et al. Implications of magnesium deficiency in type 2 diabetes: a review. Biological trace element research. May 2010;134(2):119-129.
40. Munekage E et al. Shortage and metabolic disturbance of magnesium in diabetic patients and significance of magnesium replacement therapy. Clinical calcium. Aug 2012;22(8):1235-1242.
41. Jaipakdee S et al. The effects of potassium and magnesium supplementations on urinary risk factors of renal stone patients. Journal of the Medical Association of Thailand. Mar 2004;87(3):255-263.
42. Cunningham J et al. Magnesium in chronic kidney disease Stages 3 and 4 and in dialysis patients. Clinical Kidney Journal. 2012;5(Suppl 1):i39-i51.
43. Mountokalakis TD. Magnesium metabolism in chronic renal failure. Magnesium research : official organ of the International Society for the Development of Research on Magnesium. Jun 1990;3(2):121-127.
44. Tasanarong A et al. New strategy of α- and γ-tocopherol to prevent contrast-induced acute kidney injury in chronic kidney disease patients undergoing elective coronary procedures. Nephrology, dialysis, transplantation: European Renal Association. 2013;28(2):337–44
45. Veringa SJE et al. Effect of a treatment strategy consisting of pravastatin, vitamin E, and homocysteine lowering on arterial compliance and distensibility in patients with mild-to-moderate chronic kidney disease. Clin. Nephrol. 2012;78(4):263–72
46. Saran R et al. Impact of vitamin E on plasma asymmetric dimethylarginine (ADMA) in chronic kidney disease (CKD): a pilot study. Nephrology, dialysis, transplantation: European Renal Association. 2003;18(11):2415–20
47. Minich DM et al. Acid-alkaline balance: role in chronic disease and detoxification. Alternative therapies in health and medicine. Jul-Aug 2007;13(4):62-65.
48. Fjellstedt E et al. A comparison of the effects of potassium citrate and sodium bicarbonate in the alkalinization of urine in homozygous cystinuria. Urological research. Oct 2001;29(5):295-302.
49. Tanner GA et al. Citrate therapy for polycystic kidney disease in rats. Kidney international. Nov 2000;58(5):1859-1869.
50. Ceglia L et al. Potassium bicarbonate attenuates the urinary nitrogen excretion that accompanies an increase in dietary protein and may promote calcium absorption. The Journal of clinical endocrinology and metabolism. Feb 2009;94(2):645-653.
51. Fortin MC et al. Serum concentrations and clearances of folic acid and pyridoxal-5-phosphate during venovenous continuous renal replacement therapy. Intensive care medicine. Jun 1999;25(6):594-598.
52. Shepler B et al. Update on potential drugs for the treatment of diabetic kidney disease. Clin Ther. 2012;34(6):1237–46
53. Nakamura S et al. Pyridoxal phosphate prevents progression of diabetic nephropathy. Nephrology, dialysis, transplantation: European Renal Association. 2007;22(8):2165–74
54. Post-White J et al. Advances in the use of milk thistle (Silybum marianum). Integrative cancer therapies. Jun 2007;6(2):104-109.
55. Wojcikowski K et al. Antioxidant capacity of 55 medicinal herbs traditionally used to treat the urinary system: a comparison using a sequential three-solvent extraction process. Journal of alternative and complementary medicine. Jan-Feb 2007;13(1):103-109.
56. Rastogi R et al. Long term effect of aflatoxin B(1) on lipid peroxidation in rat liver and kidney: effect of picroliv and silymarin. Phytother Res. 2001;15(4):307–10
57. Soto C et al. Effect of silymarin on kidneys of rats suffering from alloxan-induced diabetes mellitus. Phytomedicine. 2010;17(14):1090–4
58. Senturk H et al. Silymarin attenuates the renal ischemia/reperfusion injury-induced morphological changes in the rat kidney. World J Urol. 2008;26(4):401–7
59. Wenzel S et al. Effects of silibinin and antioxidants on high glucose-induced alterations of fibronectin turnover in human mesangial cell cultures. J Pharmacol Exp Ther. Dec 1996;279(3):1520-1526.
60. Launay-Vacher V et al. Prevention of cisplatin nephrotoxicity: state of the art and recommendations from the European Society of Clinical Pharmacy Special Interest Group on Cancer Care. Cancer Chemother Pharmacol. 2008;61(6):903-9.
61. Machado V et al. Carvedilol as a protector against the cardiotoxicity induced by anthracyclines (doxorubicin). Rev Port Cardiol. 2008;27(10):1277-96.
62. Bokemeyer C et al. Silibinin protects against cisplatin-induced nephrotoxicity without compromising cisplatin or ifosfamide anti-tumour activity. British journal of cancer. Dec 1996;74(12):2036-2041.
63. Karimi G et al. Cisplatin nephrotoxicity and protection by milk thistle extract in rats. Evidence-based complementary and alternative medicine : eCAM. Sep 2005;2(3):383-386.
64. El-Shitany NA et al. Silymarin prevents adriamycin-induced cardiotoxicity and nephrotoxicity in rats. Food and chemical toxicology : an international journal published for the British Industrial Biological Research Association. Jul 2008;46(7):2422-2428.
65. Abdel-Raheem IT et al. Green tea ameliorates renal oxidative damage induced by gentamicin in rats. Pakistan journal of pharmaceutical sciences. Jan 2010;23(1):21-28.
66. Khan SA et al. Studies on the protective effect of green tea against cisplatin induced nephrotoxicity. Pharmacol. Res. 2009;60(5):382–91
67. Shin BC et al. The antiproteinuric effects of green tea extract on acute cyclosporine-induced nephrotoxicity in rats. Transplant. Proc. 2012;44(4):1080–2
68. Yokozawa T et al. Green tea polyphenols and dietary fibre protect against kidney damage in rats with diabetic nephropathy. J. Pharm. Pharmacol. 2005;57(6):773–80
69. Leu J-G et al. Epigallocatechin-3-gallate combined with alpha lipoic acid attenuates high glucose-induced receptor for advanced glycation end products (RAGE) expression in human embryonic kidney cells. An. Acad. Bras. Cienc. 2013;85(2):745–52
70. Tomşa AM et al. Curcumin and Vitamin C Attenuate Gentamicin-Induced Nephrotoxicity by Modulating Distinctive Reactive Species. Metabolites. 2022 Dec 28;13(1):49.
71. El-Kader MA et alComparative nephroprotective effects of curcumin and etoricoxib against cisplatin-induced acute kidney injury in rats. Acta Histochem. 2020 May;122(4):151534.
72. Mohajeri M et al. Protective effects of curcumin against doxorubicin-induced toxicity and resistance: A review. Crit Rev Oncol Hematol. 2018 Feb;122:30-51.
73. Motaharinia J et al. Efficacy of curcumin on prevention of drug-induced nephrotoxicity: A review of animal studies. Biofactors. 2019 Sep;45(5):690-702.
74. Smirnova E et al. A Review of the Role of Curcumin in Metal Induced Toxicity. Antioxidants (Basel). 2023 Jan 21;12(2):243.
75. Trujillo J et al. Renoprotective effect of the antioxidant curcumin: Recent findings. Redox biology. 2013;1(1):448–56
76. Saldanha JF et al. Resveratrol: why is it a promising therapy for chronic kidney disease patients? Oxid Med Cell Longev. 2013;2013:963217
77. Holthoff JH et al. Resveratrol improves renal microcirculation, protects the tubular epithelium, and prolongs survival in a mouse model of sepsis-induced acute kidney injury. Kidney Int. 2012;81(4):370–8
78. Bertelli AAE et al. Resveratrol, a component of wine and grapes, in the prevention of kidney disease. Ann N Y Acad Sci. 2002;957:230–8
79. Palsamy P et al. Resveratrol protects diabetic kidney by attenuating hyperglycemia-mediated oxidative stress and renal inflammatory cytokines via Nrf2-Keap1 signaling. Biochim Biophys Acta. 2011;1812(7):719–31
80. Zhang W et al. Protective effect of resveratrol on arsenic trioxide-induced nephrotoxicity in rats. Nutr Res Pract. 2014;8(2):220–6
81. Valentovic MA et al. Resveratrol attenuates cisplatin renal cortical cytotoxicity by modifying oxidative stress. Toxicol In Vitro. 2014;28(2):248–57
82. Oktem G et al. Resveratrol attenuates doxorubicin-induced cellular damage by modulating nitric oxide and apoptosis. Exp. Toxicol. Pathol. 2012;64(5):471–9
83. Kitada M et al. Renal protective effects of resveratrol. Oxid Med Cell Longev. 2013;2013:568093.
84. Patrick L. Mercury toxicity and antioxidants: Part 1: role of glutathione and alpha-lipoic acid in the treatment of mercury toxicity. Altern Med Rev. 2002;7(6):456–71
85. Veljkovic AR et al. Protective effects of glutathione and lipoic acid against cadmium-induced oxidative stress in rat's kidney. Ren Fail. 2012;34(10):1281–7
86. Malarkodi KP et al. Prophylactic effect of lipoic acid against adriamycin-induced peroxidative damages in rat kidney. Ren Fail. 2003;25(3):367–77
87. Bae EH et al. alpha-Lipoic acid prevents cisplatin-induced acute kidney injury in rats. Nephrology, dialysis, transplantation: European Renal Association. 2009;24(9):2692–700
88. Feng B et al. The Protective Effects of α-Lipoic Acid on Kidneys in Type 2 Diabetic Goto-Kakisaki Rats via Reducing Oxidative Stress. Int J Mol Sci. 2013;14(4):6746–56
89. Li G et al. α-Lipoic acid prolongs survival and attenuates acute kidney injury in a rat model of sepsis. Clin. Exp. Pharmacol. Physiol. 2014;41(7):459–68
90. Das J et al. Mechanism of the protective action of taurine in toxin and drug induced organ pathophysiology and diabetic complications: a review. Food Funct. 2012;3(12):1251–64
91. Latchoumycandane C et al. Chronic ethanol ingestion induces oxidative kidney injury through taurine-inhibitable inflammation. Free radical biology & medicine. Apr 2014;69:403-416.
92. Sener G et al. Protective effects of taurine against nicotine-induced oxidative damage of rat urinary bladder and kidney. Pharmacology. Apr 2005;74(1):37-44.
93. Johnson DW et al. Chronic kidney disease and measurement of albuminuria or proteinuria: a position statement. Med J Aust. 2012;197(4):224–5
94. Balakumar P et al. The multifaceted therapeutic potential of benfotiamine. Pharmacol. Res. 2010;61(6):482–8
95. Karachalias N et al. Increased protein damage in renal glomeruli, retina, nerve, plasma and urine and its prevention by thiamine and benfotiamine therapy in a rat model of diabetes. Diabetologia. 2010;53(7):1506–16
96. Kihm LP et al. Benfotiamine protects against peritoneal and kidney damage in peritoneal dialysis. J. Am. Soc. Nephrol. 2011;22(5):914–26
97. Harisa GI. Benfotiamine enhances antioxidant defenses and protects against cisplatin-induced DNA damage in nephrotoxic rats. J. Biochem. Mol. Toxicol. 2013;27(8):398–405
98. Babaei-Jadidi R et al. Prevention of incipient diabetic nephropathy by high-dose thiamine and benfotiamine. Diabetes. 2003;52(8):2110–20
参考来源:
美国国立糖尿病、消化和肾病研究所
http://niddk.nih.gov
美国国家肾健康基金会
http://www.kidney.org
美国泌尿护理基金会
http://www.urologyhealth.org
加拿大肾脏健康基金会
http://www.kidney.ca
免责声明和安全信息
- 本信息(包括任何附带资料)不是为了取代医生或有关合格从业人士的建议或忠告。
- 任何人如果想要对本文涉及的药物、饮食、运动或其他生活方式的使用、或改变调整,以预防或治疗某一特定健康状况或疾病,应首先咨询医生或有关合格从业人士,并获得他/她们的许可。妊娠和哺乳妇女在使用本网站任何内容前,尤其应征求医生的意见。
- 除非另有说明,本网站所述内容仅适用于成人。
- 本网站所推荐的任何产品,消费者应该以实际的产品标签内容为准,尤其应关注重要的安全信息以及产品最新信息,包括剂量、使用方法和禁忌症等。
- 由于循证医学研究、文献及有关产品处于不断的变化中,本网站工作人员将尽力更新。
- 本网站不能保证所载文章内容、综合干预方案以及相关成分或产品述及的健康益处,也不承担任何责任。